Learners from the PAFP Foundation’s Residency Program and Community Health Center Collaborative (RPC/CHCC) gathered on a very chilly and sometimes snowy fall day at the Nittany Lion Inn in State College, Pennsylvania on Nov. 7, 2014. The Residency and Community Health Center teams came together for the third face-to-face learning session of 2014, capping off a year of interdisciplinary learning focused on quality and performance improvement education.
The November Learning Session centered around two main educational themes as a result of two great partnerships. The RPC/CHCC began an educational project with the American Cancer Society in September 2014 focusing on increasing cancer screening rates among the Collaborative teams, with a primary concentration on colorectal cancer (CRC) screening. The teams were offered clinical assistant training with three regional advanced patient-centered medical home training sessions presented by the Pittsburgh Regional Health Initiative, as well as the CoachClinic® with the National Society of Health Coaches, where learners enjoyed an interactive day of learning and exploring patient engagement, motivational interviewing, and other health coach skills. These great educational activities culminated at the Learning Session with the interdisciplinary teams coming together for a morning of excellent CRC education and tools provided by the American Cancer Society.
The afternoon of Nov. 7 also served as the kick-off event for a weight management project that the Collaborative will take part in through late 2015, in partnership with the Joslin Diabetes Center. The Joslin Diabetes Center faculty introduced the scope of the “obesity challenge” and offered tools and strategies for nutritional management and exercise therapy. This education will continue through a variety of virtual clinics and educational activities during RPC/CHCC team calls. The Collaborative teams will continue to submit monthly data to the PAFP Foundation on both body mass index and cancer screenings, as well as diabetes, smoking and depression measures, to assess the impact of all of these interdisciplinary projects.
The RPC/CHCC teams combined for an audience of approximately 100 clinical and non-clinical learners for this one-day Learning Session. Teams created rapid-response action plans (PDSAs) based on the education provided at the conference; they’ll implement the PDSAs back home in their practices, involving the whole practice staff and spreading the learning to a larger audience.
Tweets
The PAFP Foundation’s effort to expand the educational reach of all live events includes encouraging faculty members, staff and attendees to actively spread key messages on Twitter during these live sessions. Here is a sampling of their tweets and some notes from select lectures.
TOPICS: Colorectal Cancer Screening | Weight Management | Exercise is Medicine
COLORECTAL CANCER SCREENING
FIT outreach (40%) was superior to colonoscopy outreach and usual care (12%) for improving CRC screening rates.
ACS has 100 staff across the country supporting primary care practices in their cancer screening improvement efforts.
You must enlist patient preference. Must be less paternalistic in our approach.
Great lecture on CRC at State College PCMH conference.
PA CRC screening are ok. Practices a little above average. CHC rates a little below. We want to be better than average!
Colon cancer has the 3rd leading cancer deaths.
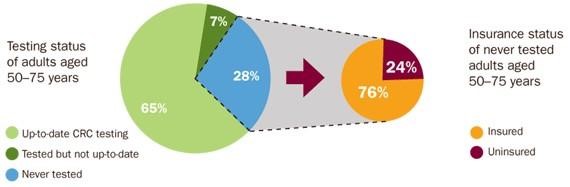
Lack of colon cancer screening is not just a lack of insurance. 76% unscreened are insured.
Dr. Durado Brooks: 95% of colon cancers will be missed by a single stool hemoccult test. It's time to stop this practice!
If we screen for colon cancer, survival rates are MUCH better by catching it early.
Helpful toolkit to increase cancer screening rates in primary care: http://goo.gl/lOaGJ1
46% patients studied with normal colonoscopy had unneeded repeat within 7 years.
Get your patients screened for colon cancer with this educational video from the American Cancer Society: http://goo.gl/WyOxYg
Use wall chart for colon cancer screening. Give patients something to view while wait: http://goo.gl/bbxyYd
WEIGHT MANAGEMENT
Dr. Osama Hamdy: Waist circumference is correlated with presence of visceral fat and increased risk of cardiovascular events.
Type II diabetes in children is on the rise.
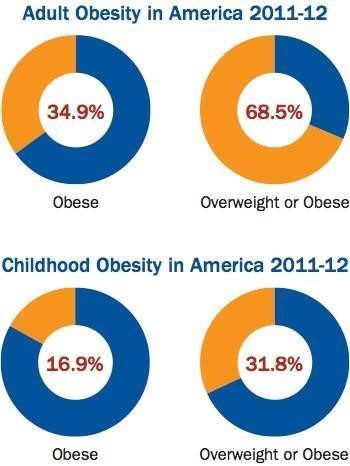
There are 12 million obese children in US and 23% of obese children have type 2 diabetes.
78.1 million adult Americans are obese.
The prevalence of obesity is staggering.
Serotonin can go up or down when you eat.
Sleep deprivation ---> obesity, insulin resistance and downward spiral. Always ask about sleep.
The key for weight loss success is motivating the patient.
National Weight Control Registry: Patients who lost > 30 lbs and kept off for 1 yr . 38% weighed themselves daily. 78% ate breakfast daily.
Tracking what you eat will result in reduced intake.
CMS will pay for up 20 encounters per year for weight loss counseling. If BMI is measured, CMS will pay for weekly visits x 4.
Reviewing the stages of change in relation to obesity:
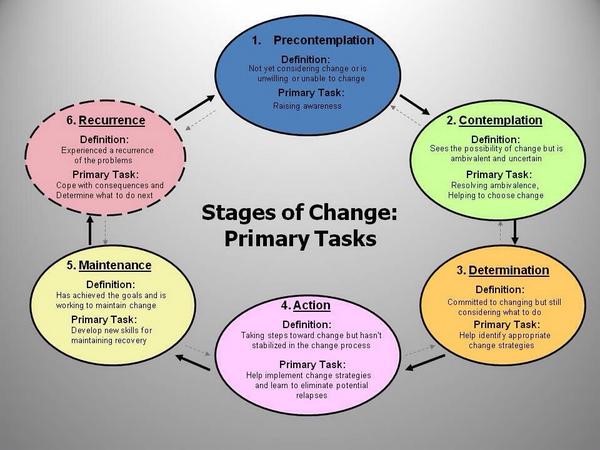
Using self-plans for weight loss. Importance + confidence = readiness.
Everything's fine- wrong answer if you’re diabetic.
Dr. Hamdy: Use nutrition as therapy. Individual assessment, assist with lifestyle management, modify diet.
Obesity management advice should not come from Homer Simpson.

The key to any weight loss is you have to keep the carbs down.
University of Washington School of Medicine has a nice patient education handout on glycemic index: http://goo.gl/GbmgXD
Want a potato, go sweet potato; you want pasta, get fiber. Restrict carbs. Structure plate with a plan:

Keep them motivated on every accomplishment!
VFW-veggies, fruits and whole grains. Formula for weight loss.
EXERCISE IS MEDICINE
In the battle against sarcopenia, obesity and diabetes, consider exercise as medicine.
In patients with physical limitations to exercise, consider this. http://goo.gl/IIoEBn
FIIT Principle - Frequency, Intensity, Type of Exercise, Time.